J Child Psychol Psychiatry. 2005 Jun;46(6):572-9
***This is a very interesting study. The written work-up of the study is very misleading and untrue. See if you can spot the falsehood in the study.***
The study abstract is below:
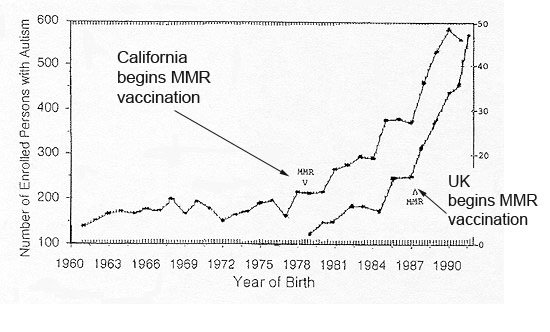
BACKGROUND: A causal relationship between the measles, mumps, and rubella (MMR) vaccine and occurrence of autism spectrum disorders (ASD) has been claimed, based on an increase in ASD in the USA and the UK after introduction of the MMR vaccine. However, the possibility that this increase is coincidental has not been eliminated. The unique circumstances of a Japanese MMR vaccination program provide an opportunity for comparison of ASD incidence before and after termination of the program. METHODS: This study examined cumulative incidence of ASD up to age seven for children born from 1988 to 1996 in Kohoku Ward (population approximately 300,000), Yokohama, Japan. ASD cases included all cases of pervasive developmental disorders according to ICD-10 guidelines. RESULTS: The MMR vaccination rate in the city of Yokohama declined significantly in the birth cohorts of years 1988 through 1992, and not a single vaccination was administered in 1993 or thereafter. In contrast, cumulative incidence of ASD up to age seven increased significantly in the birth cohorts of years 1988 through 1996 and most notably rose dramatically beginning with the birth cohort of 1993. CONCLUSIONS: The significance of this finding is that MMR vaccination is most unlikely to be a main cause of ASD, that it cannot explain the rise over time in the incidence of ASD, and that withdrawal of MMR in countries where it is still being used cannot be expected to lead to a reduction in the incidence of ASD.
Below is the graph from this study:
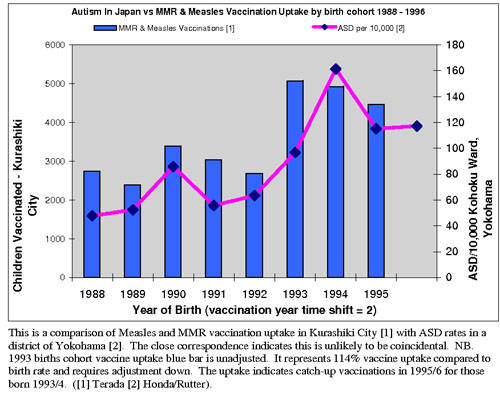
***This graph shows two things. The blue bars show the number of children in Japan that were vaccinated during a particular year in the study. The pink curve shows the incidence of autism during the same periods. As the number of children that were vaccinated INCREASED (1988-1993), the number of children with autism also INCREASED. As the number of children that were vaccinated DECREASED (1993-1996), the rate of autism also DECREASED. This is a DIRECT CORRELATION between autism rates and the vaccinations used.***
Did you find the misleading statements in the study?
The authors of the study state NO correlation. The results of the graph CLEARLY show a correlation.
The authors were very crafty in their conclusion. They state that "MMR vaccination is most unlikely to be the main cause of ASD". Anyone looking at the study's graph would conclude the opposite. There is an ABSOLUTE correlation between autsim and MMR vaccination rates.
In the study's "RESULTS" section, it says that "The MMR vaccination rate in the city of Yokohama declined significantly in the birth cohorts of years 1988 through 1992". It did? Am I looking at the same information that these researchers are? It looks like there was a slight upward trend in MMR vaccination rate from 1988-1992. There was NO "significant decline" as they stated.
Also in the "RESULTS" section, they state that "not a single vaccination was administered in 1993 or thereafter". NOT ACCORDING TO THE GRAPH! In 1993 there were around 5000 children vaccinated and the following 2 years showed a decline in the number of children receiving vaccines for MMR. So to say that "not a single vaccination was administered" is not true according to their information in the graph.
When the truth stares you in the face, they still try to cover up direct connections. Why? Follow the money.
«« Back to Top »»